Get Ready for Better Results!
Less Crumple. More Control. Optimized Fit.
We’ve updated our classic fit gutta percha to perform better! The new version includes a thinner design to ensure a precise apical fit.

Features
Improved Navigation
Slimmer profile allows Gutta Percha to drop to length without hangups in the canal curvature. No more binding in canals due to taper.

Seamless Integration
Tailored to work effortlessly with EdgeEndo file systems for streamlined endodontic procedures.

Proprietary Stiffening Process
Provides improved handling, less tip crumpling, and improved displacement of sealer.

Optimized Apical Fit with Coronal Venting
Designed for a tight apical fit with extra space in the coronal third to facilitate the upward venting of sealer thus minimizing the risk of apical extrusion.
Shop Gutta Percha by File System
| File System | Improved Gutta Percha | Improved Paper Points |
|---|---|---|
| EdgeOne Platinum | EdgeEndo .06 | EdgeEndo .06 |
| EdgeOne Fire | EdgeOne Fire | EdgeOne Fire |
| EdgeOne Blaze Utopia | EdgeOne R Utopia | EdgeOne Fire or EdgeEndo .06 |
| EdgeTaper | EdgeTaper | EdgeTaper |
| EdgeTaper Platinum | EdgeTaper | EdgeTaper |
| EdgeTaper Blaze Utopia | EdgeTaper | EdgeTaper |
| EdgeDiamond Utopia | EdgeTaper | EdgeTaper |
| Universal .04 | EdgeEndo .04 | EdgeEndo .04 |
| EdgeSequel Sapphire .04 | EdgeEndo .04 | EdgeEndo .04 |
| EdgeSequel Utopia .04 | EdgeEndo .04 | EdgeEndo .04 |
| EdgeV-Taper HT | EdgeEndo .04 | EdgeEndo .04 |
| Universal .06 | EdgeEndo .06 | EdgeEndo .06 |
| EdgeSequel Sapphire .06 | EdgeEndo .06 | EdgeEndo .06 |
| EdgeSequel Utopia .06 | EdgeEndo .06 | EdgeEndo .06 |
| EdgeFile X3 .04 | EdgeFile X7 .04 | EdgeEndo .04 |
| EdgeFile X3 .06 | EdgeFile X7 .06 | EdgeEndo .06 |
| EdgeFile X7 .04 | EdgeFile X7 .04 | EdgeEndo .04 |
| EdgeFile X7 .06 | EdgeFile X7 .06 | EdgeEndo .06 |
| EdgeEvolve | EdgeEndo .04 or EdgeEndo .06 | EdgeEndo .04 or EdgeEndo .06 |
Case Study 1
A 72-year-old male presented for evaluation and treatment tooth #5 (Dx: necrosis, symptomatic apical periodontitis). His dentist noted periapical radiolucency associated with the mesial apical third. The tooth had previously been restored with multiple resin restorations and is indicated for full coverage crown. Intraoral exam revealed no soft tissue findings or mobility.
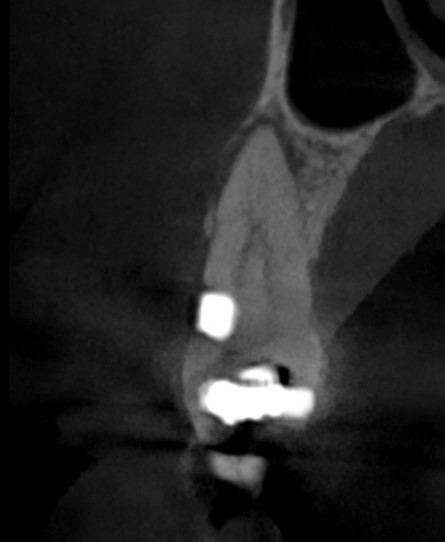
Pre-operative PA radiograph shows a “fast-break” in the apical third, suggestive of multiple canals. CBCT revealed a 2:1:2 morphology with a mesial dilaceration in the apical third, explaining the eccentric nature of the PARL to the mesial. The buccal resin appeared to closely encroach or even occlude the buccal canal.
EdgeFile X7 files were selected for this case, with attention given to the atypical canal morphology and apical curvature. The canals were confirmed necrotic upon access. EdgeFile X7 17.06 was used to pre-flare the orifices. Small hand files were then scouted in the apical third to patency. EdgeV-Taper HT 14.03 was used as a glidepath file to ensure both canals were patent. EdgeFile X7 17.04 was taken to length with relative ease under chamber flooded with EDTA. The canals were then relatively easily negotiated with EdgeFile X7 25.04 and 30.04 files. Active ultrasonic irrigation of EDTA and NaOCl was done for one minute per canal.
The canals were then dried, and EdgeFile X7 30.04 cones were confirmed to seat to length. The tooth was obturated with two EdgeFile X7 30.04 cones and BC sealer using a hydraulic obturation technique. Post-op radiograph confirmed good apical seal and patency and reinforces that the portal of exit is frequently not confluent with the radiographic apex, but often eccentric. The patient will return to his dentist for full coverage restoration.
Zak James, DMD
Diplomate of the American Board of Endodontics • Trained at Harvard, MUSC & UT Health San Antonio
Concord, NC


Case Study 2
A 63-year-old male patient presented for evaluation #3 (Dx: necrosis, symptomatic apical periodontitis). No soft tissue findings were noted, and the tooth was positive to percussion. A large DO amalgam was present extending subgingivally, but without probing.
Pre-operative imaging demonstrated periapical radiolucencies associated with all three apices. The MB root was shown to have severe apical dilaceration, while the DB canal also dilacerates in the apical third. The patient presented with limited opening, presenting a challenge both for access and instrumentation given the apical anatomy.
EdgeFile X7 files were selected for this case due to their flexibility, shape memory, and conservative taper. The tooth was accessed and confirmed necrotic without evidence of fractures. Four canal orifices were located. EdgeFile X7 17.06 was used to pre-flare the canals to resistance. Under generous EDTA irrigation, EdgeV-Taper HT 14.03 was taken to resistance. Small hand files confirmed patency and working lengths with electronic apex locator. 25 mm EdgeFile X7 17.04 was worked with 14.03 EdgeV-Taper HT in a crown-down manner to achieve a glide path. The DB canal required handfiling in the apical third before glide path could be passively achieved with rotaries. Once 17.04 was worked to length, the canals were enlarged in step-back fashion using EdgeFile X7 25.04 and 30.04, with 40.04 in the palatal canal. Canals were irrigated with passive ultrasonics.
EdgeFile X7 GP cones were selected for obturation. Cones were sized to their corresponding master X7 rotary file. A cone shot with BC sealer confirmed patency and apical seat in all canals; MB2 remained a separate canal, exiting slightly shorter than the main MB canal. Orifices were sealed with BC liner, yellow teflon placed with EdgeTemp temporary. The patient will return to his dentist for full coverage restoration.
Zak James, DMD
Diplomate of the American Board of Endodontics • Trained at Harvard, MUSC & UT Health San Antonio
Concord, NC



Testimonials
“These gutta-percha cones represent a substantial improvement. The .04 taper reveals enhanced adaptation to the prepared canal geometry, resulting in a more accurate apical and lateral seal and reducing the likelihood of voids during obturation.”
– Dr. Jason Foreman
“I’m impressed with the new X7 Gutta Percha points. They exhibit superior canal conformity and provide a more precise and predictable obturation with the X7 system compared to conventional gutta-percha points.
With the new EdgeFile X7 Gutta Percha Points, I immediately found that there is no guesswork in how to obturate. They seat with good apical tug-back at working length and consistently to my reference point. I need fewer gutta-percha points now because these essentially it any shape that I prepare-the first time and every time.“
– Dr. Zak James
FAQs
The new gutta percha is noticeably thinner than the previous product we used. Why was this done and will it cause me to have to buy more product?
Only the coronal portion of the new gutta percha has received a design revision. This was done following feedback from numerous clinicians that the previous GP was unable to reach full working length. In longer canals the previous gutta percha would consistently get “hung up” and come up short of working length. See the image below. The design of the new gutta percha also features an improved apical fit that more closely matches the file design. Therefore, the number of gutta percha cones used per case would be identical to previous obturation techniques. Most doctors are now using bioceramic sealers which do not shrink and bond to the dentin. In years past there was more focus on compacting gutta percha and taking up the maximum amount of space in the canal with the gutta percha because the sealers shank considerably and did not bond. By using a bioceramic sealer you can now rely on the sealer to achieve three primary functions.
- Take up some space in the canal which is less expensive than filling the entire canal with sealer.
- Provide a hydraulic piston to help drive the sealer into the canal anatomy and apical intricacies.
- Provie a pathway for retreatment should the case fail for whatever reason.
It is important to understand that gutta percha in the modern day of bonded bioceramic obturation only achives the above three functions. In the past we had very large gutta percha and took a lot of time flare the canal to facilitate the placement and compaction of gutta percha but now we simply need to use a cone to achieve the above three functions and we can allow the bioceramic sealer to bond to the canal and do its job. To seal the root canal.
How is it different than the gutta percha points I have been using?
This conservative coronal taper serves multiple purposes. It encourages the upward flow of sealer, so sealer flows up and out rather than out and down, thus reducing the risk of apical extrusion. The conservative nature also supports minimally invasive shaping techniques which have gained significant traction by clinicians and eliminates getting hung up in curvatures or conservative canal shapes.
Will I need to use more sealer? Do I need to compensate for sealer shrinkage?
The amount of sealer needed to properly seal the canal is highly dependent on the shaping technique and the natural anatomy and any change in volume needed will not be significantly relevant. Sealer can be expressed directly into the canal or utilizing a cone coating technique, regardless of application the final gutta percha point should be inserted slowly into the canal to encourage hydraulic flow of sealer. We are proud to offer three choices when it comes to Bioceramic sealers. All of which exhibit zero shrinkage. Our newest sealer, EdgeUtopia Bioceramic Sealer is our high-quality sealer option that touts an over 50% cost savings per gram compared to our other BC Sealer options. Generally you will use more sealer than you did in the past with a resin on ZOE sealer. Those sealers shrank and the primary concern during obturation was to “minimize the sealer interface”. When a sealing material shinks and is not as biocompatible it makes sense to take extra time, cost and effort to fill the canal with gutta percha but once you solve that issue you no longer have to worry about compaction. Let the sealer do its job. Many doctors actually prefer to have the sealer completely surround the cone once they understand that he sealer doesn’t shink and it bonds to the dentin while also providing a biological benefit (high pH to kill bacterial and osteogenic properties). It is a bit of a paradigm shift in endo and the reason why all of the NiTi companies are now promoting minimally invasive shaping systems. Now that we solved the issue with the sealer shrinking and losing its bond over time we can finally shape the canal as minimally as necessary to promote the debridement and killing of bacteria and then let the sealer do its work.
Is the sizing the same or do I need to size up?
There is no need to size up. In fact, the new gutta percha have been optimized to ensure a snug apical fit. Simply select the point that corresponds to your finishing file.
Does this gutta percha include new ingredients?
The ingredients consist of Gutta Percha, Zinc Oxide, Zirconium Oxide, Barium Sulfate and a Coloring Agent.
How will this new gutta percha help improve my cases?
While we can’t guarantee an improvement in cases we can suggest you will experience an improvement in workflow now that certain frustrations have been reduced with the new design. Enjoy a reduction in tip crumpling and mid-canal binding thanks to the conservative shape and proprietary stiffening process.
How will this gutta percha perform during the removal and retreatment of obturated canals?
Like all gutta percha, our new gutta percha provides the pathway for retreatment should retreatment become necessary. There will be no difference in removal processes and procedures using this gutta percha as compared to any other gutta percha.
Improved Paper Points
- Highly absorbent
- Clear millimeter reference marks
- Specifically tapered to match corresponding finishing file
- Universal .04 and .06 available
